We Believe Your Body Can Function As It Was Meant To
Guiding You to Wellbeing with Functional and East Asian Medicine
We Believe Your Body Can Function As It Was Meant To
Guiding You to Wellbeing with Functional and Traditional Chinese Medicine
East Asian Medicine is the Original Functional Medicine
At Guide to Wellness, we use a simple Three-Step Process to deliver an integrated, comprehensive and holistic approach to health and wellbeing.
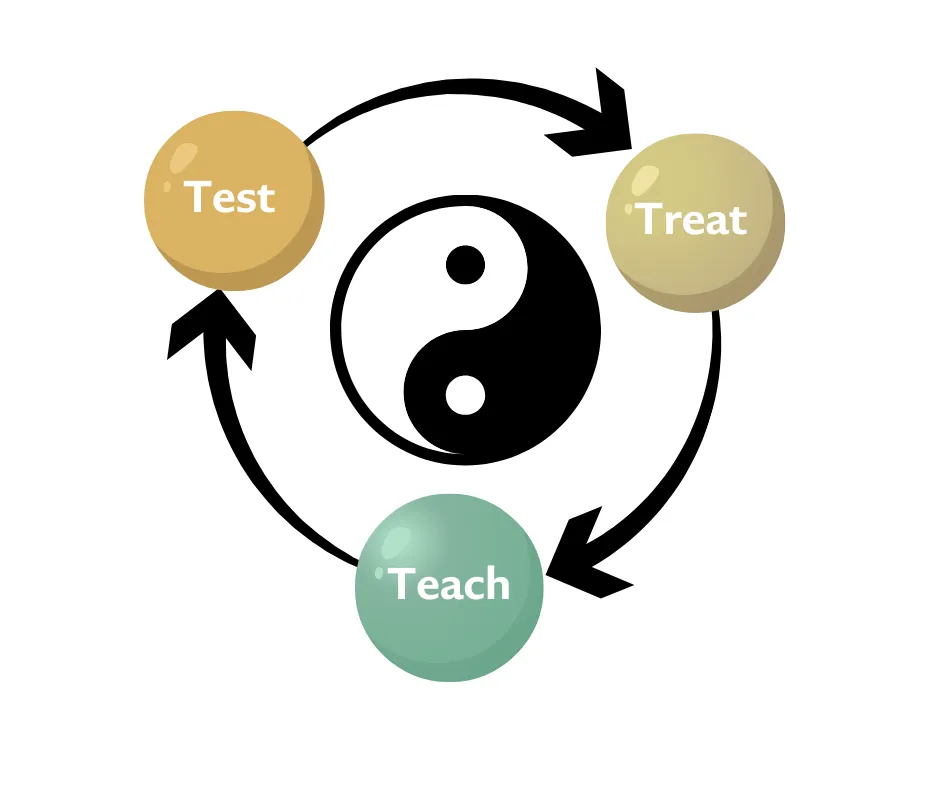
Test
Imagine unlocking the secrets of your health that have been holding you back. Through our thorough evaluations and assessments, you'll discover the underlying factors affecting your wellbeing. We provide crucial insights into your unique biochemistry and symptoms, empowering you with a personalized health approach designed just for you.
Treat
This is where true healing is your new reality. With insights from your lab tests and assessments, we craft personalized treatment plans that address the root causes of your health conditions. Our focus is on restoring your body’s natural balance, ensuring you experience long-lasting wellness and vitality.
Teach
Empowerment is at the heart of your journey with us. We equip you with the tools and knowledge to create lasting lifestyle changes. Through personalized coaching and guidance, you’ll find the support you need to achieve optimal health and embrace life at its fullest potential.
Pillars of Your Optimal Health Journey

Digestion & Detoxification
Your digestive health is vital to your overall well-being. In the Test phase, we’ll evaluate your gut health by analyzing stool samples and liver function to uncover any imbalances or triggers. The Treat phase provides you with a personalized plan designed to restore gut health and enhance detoxification, using herbal remedies, dietary adjustments, and nutritional support. Finally, in the Teach phase, you’ll gain the knowledge to maintain a healthy diet, stay properly hydrated, and incorporate lifestyle habits that promote optimal digestion and detoxification.
Functional Nutrition
Nourishing your body with the right nutrients is key to your health. In the Test phase, we’ll assess your blood chemistry, examine your dietary habits, and evaluate your metabolic function to identify any nutritional gaps or imbalances. Moving to the Treat phase, we’ll create a customized nutrition plan that fits your unique needs, including guidance on whole foods, supplements, and meal timing to optimize your health. In the Teach phase, you’ll learn about mindful eating, how to balance micro and macronutrients, and specific strategies to support your foundational health through better nutrition.

Hormonal & Metabolic Health
Achieving balance in your hormones and metabolism is essential for your energy, mood, and overall vitality. During the Test phase, we’ll dive into your hormonal and metabolic health, using comprehensive assessments to pinpoint any imbalances. In the Treat phase, you’ll receive a personalized plan to restore balance, which may include targeted nutrition, supplementation, and lifestyle changes tailored just for you. In the Teach phase, we’ll empower you with knowledge and strategies to maintain hormonal and metabolic health, so you can enjoy consistent energy and well-being.
Rest and Movement
Your health thrives on quality rest and regular movement. In the Test phase, we’ll evaluate your sleep patterns, stress levels, and physical fitness to identify areas where you might need support. The Treat phase is where you’ll receive a tailored plan to improve your sleep, relaxation, and physical strength. This could include herbal remedies, nutritional supplements, and techniques like acupuncture. In the Teach phase, you’ll learn how to incorporate mindfulness, relaxation techniques, and consistent physical activity into your daily life, ensuring lasting improvements in your rest and movement.

Brain Health & Well-being
Your mental and emotional well-being are just as important as your physical health. In the Test phase, we’ll assess your brain health by analyzing neurotransmitter function, stress levels, and inflammation markers to uncover any underlying issues. The Treat phase is where you’ll benefit from a customized plan that may include herbal remedies, supplements, acupuncture, and stress-reduction techniques aimed at enhancing your brain health and emotional well-being. In the Teach phase, you’ll be equipped with mindfulness practices, positive psychology tools, and self-care strategies to support your brain function and overall happiness.
Transformative Treatments for Your Wellness

Wellness Planning
Your journey to optimal health starts with a personalized wellness plan crafted just for you. We integrate acupuncture, nutrition, herbal medicine, and collaborate with other healthcare professionals to address the root causes of your health concerns. Our holistic approach ensures you receive individualized care that’s tailored to your unique needs, helping you achieve your fullest potential for wellness.

Acupuncture
Feel the revitalizing effects of acupuncture, designed to restore balance and enhance your body’s energy flow. Using fine, sterile needles, we gently stimulate specific points to improve the circulation of energy (Qi) and blood throughout your body. Whether you’re seeking relief from complex health conditions or simple pain, acupuncture treatments are customized to support your overall well-being and restore your body’s natural equilibrium.

Herbal Medicine
Experience the power of herbal medicine, a cornerstone of Traditional Chinese Medicine, to support your health. Our extensive range of Chinese herbs and whole food-based nutritional supplements is carefully selected to address your specific needs. These herbs not only help to eliminate disease but also nourish and balance your body, enhancing organ function and strengthening your immune system for improved overall health.

Nutritional Guidance
Unlock the benefits of personalized nutritional guidance tailored to your evolving needs. We focus on creating well-balanced lifestyle choices that strengthen your digestion, boost your energy, and promote longevity. Our collaborative approach with other healthcare providers allows us to design a program that addresses everything from your diet and exercise to stress and sleep management, giving you the tools to live your best life every day.
Work With Us
New Patients: Fill Out This Form And Our Associate Will Get In Touch With You Within 1 Business Day
Existing Patients Please Use the Patient Portal